Hearing the words “brain tumor” can be frightening for any patient or family. However, not every brain tumor carries a grim prognosis. In fact, Grade I Pilocytic Astrocytoma stands as one of the most treatable and least aggressive tumors that can develop within the central nervous system. For many patients, particularly children, this diagnosis comes with genuine hope and, in most cases, an excellent chance of long-term cure.
Throughout this guide, we will walk through every aspect of pilocytic astrocytoma, starting from its underlying biology and moving through the symptoms that bring patients to medical attention, the diagnostic workup, and the treatment strategies that offer the best outcomes. Whether you are a newly diagnosed patient, a parent seeking answers, or a healthcare professional looking for a detailed reference, this article has been written with you in mind.
In This Article
- What Is Grade I Pilocytic Astrocytoma?
- Epidemiology and Risk Factors
- Types and Common Locations
- 10 Symptoms You Should Recognize
- Diagnosis: From Clinical Exam to Molecular Testing
- The WHO Brain Tumor Grading System
- Treatment Options Overview
- Microsurgical Resection: The Gold Standard
- Chemotherapy, Radiation and Targeted Therapy
- Prognosis and Survival Data
- Pilocytic Astrocytoma vs. Glioblastoma
- Long-Term Outlook and Follow-Up
- Expert Insight: Prof. Dr. Serdar Baki Albayrak
- Frequently Asked Questions
What Is Grade I Pilocytic Astrocytoma?
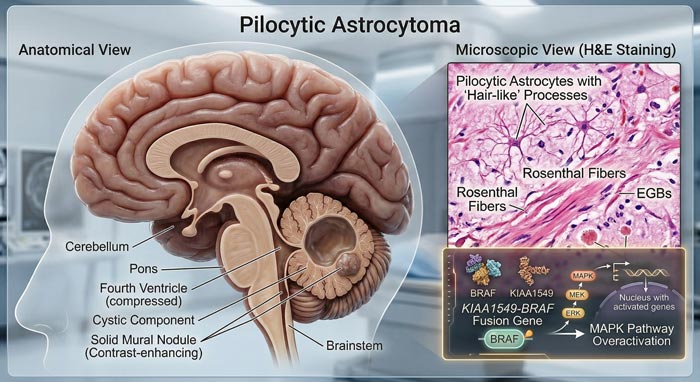
To put it simply, pilocytic astrocytoma (PA) is a slow-growing brain tumor that the World Health Organization classifies as a Grade I glioma, the lowest and most benign tier in its four-level grading system. The name itself offers a clue about what pathologists see under the microscope: “pilocytic” derives from the Greek word pilos, meaning hair-like, because the tumor cells have long, thin projections that resemble strands of hair.
What makes this tumor fundamentally different from more aggressive brain cancers is its growth behavior. Unlike glioblastoma multiforme (GBM), which infiltrates and destroys surrounding tissue at an alarming pace, pilocytic astrocytoma tends to grow as a self-contained mass with clear borders. As a result, neurosurgeons can often separate it from normal brain tissue during surgery, which is precisely why complete removal, and therefore cure, is realistic for the majority of patients.
Core Features at a Glance
- Growth Pattern: Slow-growing, well-circumscribed margins that do not infiltrate healthy tissue
- WHO Classification: Grade I – the most benign category of brain tumors
- Cell of Origin: Astrocytes, the star-shaped glial cells responsible for supporting neurons
- Classic MRI Appearance: A cystic mass paired with a brightly enhancing solid nodule
- Key Molecular Marker: KIAA1549-BRAF fusion, found in roughly 70 to 80 percent of cases
- Risk of Becoming Malignant: Extremely low; fewer than 2 percent ever progress to a higher grade
Under the microscope, pathologists look for two signature findings that confirm the diagnosis. First, they search for Rosenthal fibers – thick, corkscrew-shaped protein deposits found in the compact areas of the tumor. Second, they identify eosinophilic granular bodies within the looser, more sponge-like regions. When both features appear together in what pathologists call a “biphasic pattern,” the diagnosis becomes straightforward.
Who Gets Pilocytic Astrocytoma? Epidemiology and Risk Factors
Pilocytic astrocytoma holds the distinction of being the most common brain tumor in the pediatric population, accounting for about 15 to 20 percent of all central nervous system tumors diagnosed in children. While it primarily affects kids and teenagers, it is worth noting that adults can develop this tumor as well, although such cases are considerably less frequent.
Key Statistics
| Parameter | Details |
|---|---|
| Peak Age of Onset | 5 to 15 years |
| Gender Distribution | Slight male predominance (1.1 to 1) |
| Annual Incidence | 0.37 per 100,000 people |
| Share of Pediatric CNS Tumors | 15 to 20 percent |
| Share of All Gliomas | Approximately 5.4 percent |
| Known Genetic Association | Neurofibromatosis Type 1 (NF1) |
What Causes It?
In most cases, the exact trigger behind pilocytic astrocytoma remains unknown. Nevertheless, one well-documented risk factor stands out: Neurofibromatosis Type 1 (NF1), a genetic disorder caused by mutations on chromosome 17. Children who carry this mutation face a significantly higher chance of developing optic pathway gliomas, which are frequently pilocytic astrocytomas.
Beyond NF1, however, there is no strong evidence linking pilocytic astrocytoma to environmental exposures, dietary habits, or lifestyle choices. Consequently, parents should understand that this tumor is not something they could have prevented. It arises from spontaneous genetic changes during cell growth rather than from any external cause.
Types and Common Locations
One of the most clinically important aspects of pilocytic astrocytoma is where it develops. The tumor location directly shapes the symptoms a patient experiences, determines the surgical approach, and ultimately influences the prognosis. With that in mind, let us look at the five most frequent sites.
- Cerebellum (Posterior Fossa): This is by far the most common location, representing roughly 60 percent of all cases. Because the cerebellum sits at the back of the brain and controls coordination, patients often present with balance difficulties. On the positive side, cerebellar tumors tend to be highly accessible for surgical removal, which is why they carry the best overall prognosis.
- Optic Pathway and Hypothalamus: The second most frequent site, especially among children with NF1. Since these tumors grow along the optic nerves or near the brain’s hormonal control center, they can lead to gradual vision loss or endocrine disruptions. Due to the critical structures involved, complete surgical removal is often not feasible in this location.
- Brainstem: Brainstem pilocytic astrocytomas typically grow outward (exophytically) from the surface rather than burrowing deep inside. This growth pattern is important because it distinguishes them from diffuse intrinsic pontine glioma (DIPG), a far more aggressive tumor. Thanks to their outward growth, many brainstem PAs can be safely approached surgically.
- Cerebral Hemispheres: While less common in children, hemispheric pilocytic astrocytomas appear more frequently in adult patients. These tumors may cause seizures or focal neurological symptoms depending on their precise location within the brain’s functional areas.
- Spinal Cord: The least common location overall, spinal cord PAs can produce progressive weakness, sensory changes, and difficulties with bladder or bowel control. Although the spinal cord is a delicate structure, experienced neurosurgeons can often achieve meaningful tumor reduction.
10 Symptoms of Pilocytic Astrocytoma You Should Recognize
Because pilocytic astrocytoma grows slowly, its symptoms tend to creep in gradually over weeks or even months rather than appearing suddenly. This gradual onset sometimes delays diagnosis, particularly in young children who cannot clearly describe what they are feeling. For that reason, awareness of the warning signs is essential.
Pilocytic Astrocytoma Warning Signs and Symptoms
1. Persistent Headaches
These headaches often peak in the early morning or wake children from sleep. They differ from ordinary tension headaches because they worsen steadily over time and may be accompanied by other neurological symptoms.
2. Nausea and Vomiting
Projectile vomiting, particularly in the morning and sometimes without preceding nausea, is a classic red flag for elevated pressure inside the skull. When a child vomits repeatedly upon waking, it warrants prompt medical evaluation.
3. Balance and Coordination Problems (Ataxia)
This symptom is especially common when the tumor sits in the cerebellum. Parents may notice their child becoming unusually clumsy, stumbling frequently, or struggling with activities that require fine motor control such as handwriting.
4. Vision Changes
Blurred vision, double vision, or a slow narrowing of the visual field can develop when the tumor involves the optic pathway. In some cases, these changes are first picked up during routine eye exams rather than reported by the patient.
5. Papilledema
This refers to swelling of the optic disc at the back of the eye, visible during a standard fundoscopic examination. It signals increased intracranial pressure and should always trigger urgent neuroimaging.
6. Seizures
Seizures are more likely when the tumor grows within the cerebral hemispheres. They may be focal (affecting one part of the body) or generalized, and in adult patients they are sometimes the very first symptom that leads to diagnosis.
7. Behavioral and Cognitive Shifts
Teachers or parents might observe personality changes, unexpected irritability, falling grades, or unusual fatigue. In toddlers, previously acquired milestones such as walking or talking may begin to regress.
8. Endocrine Disruptions
When the tumor develops near the hypothalamus, it can interfere with hormone production, leading to early puberty, stunted growth, excessive thirst and urination (diabetes insipidus), or unexplained weight gain.
9. Head Tilt (Torticollis)
Children with posterior fossa tumors sometimes adopt a persistent head tilt. This serves as an unconscious adjustment to maintain cerebrospinal fluid flow and reduce pressure symptoms.
10. Increased Head Size (Macrocephaly)
In infants whose skull bones have not yet fused, blocked cerebrospinal fluid drainage can cause the head to enlarge noticeably. Pediatricians monitor head circumference at every well-child visit partly for this reason.
If you recognize several of these signs in yourself or your child, it is important to seek neurological evaluation without delay. Early detection can make a meaningful difference in treatment planning and outcomes. Reach out to our team for a specialized consultation.
Diagnosis: From Clinical Exam to Molecular Testing
Reaching a definitive diagnosis of pilocytic astrocytoma involves a carefully layered process. Each step builds on the previous one, moving from bedside assessment to advanced imaging and finally to laboratory analysis of the tumor tissue itself.
Step 1 – Neurological Examination
The journey typically begins with a thorough neurological exam. The clinician tests cranial nerve function, motor strength, reflexes, coordination, and cognitive ability. In pediatric patients, the assessment also includes developmental milestones and head circumference measurements, both of which may reveal subtle abnormalities.
Step 2 – Neuroimaging
MRI with gadolinium contrast remains the single most informative imaging study for pilocytic astrocytoma. On MRI, the tumor usually appears as a well-defined cystic mass with a brightly enhancing solid nodule. This pattern is so characteristic that experienced neuroradiologists can often suggest the diagnosis before surgery ever takes place.
Several MRI features help distinguish PA from other brain tumors:
- Clear, well-circumscribed borders with little or no surrounding edema
- Hypointense cyst and enhancing nodule on T1-weighted sequences
- Hyperintense signal throughout on T2/FLAIR sequences
- No restricted diffusion on DWI, a finding that separates it from more aggressive lesions
In addition to standard MRI, advanced techniques such as MR spectroscopy (which reveals metabolic signatures), perfusion imaging (which maps blood flow), and diffusion tensor imaging (which traces white matter pathways) can provide extra layers of information that guide surgical planning.
Step 3 – Tissue Diagnosis
Although imaging offers strong clues, the definitive diagnosis always requires examination of tumor tissue obtained either through surgical resection or a targeted biopsy. The neuropathologist looks for the hallmark biphasic pattern, Rosenthal fibers, eosinophilic granular bodies, and, critically, the absence of significant mitotic activity.
Step 4 – Molecular Profiling
Modern neuropathology goes beyond what can be seen under the microscope. Molecular testing now plays a central role in confirming the diagnosis and can also guide treatment decisions. The KIAA1549-BRAF fusion is present in around 70 to 80 percent of pilocytic astrocytomas and serves as a molecular fingerprint for the tumor. Meanwhile, the BRAF V600E point mutation, found in a smaller subset, has therapeutic significance because it can be targeted with specific inhibitor drugs. Importantly, IDH mutations, which define diffuse gliomas, are absent in pilocytic astrocytoma, helping to confirm the Grade I classification.
Understanding the WHO Brain Tumor Grading System
To appreciate where pilocytic astrocytoma sits within the broader landscape of brain tumors, it helps to understand the WHO grading framework. This system classifies astrocytic tumors on a four-tier scale based on their microscopic appearance, growth behavior, and molecular characteristics.
| WHO Grade | Tumor Type | Behavior | Typical Prognosis |
|---|---|---|---|
| Grade I | Pilocytic Astrocytoma | Slow-growing, well-circumscribed | Excellent (over 95% at 10 years) |
| Grade II | Diffuse Astrocytoma | Slow-growing but infiltrative | Good (5 to 10+ years) |
| Grade III | Anaplastic Astrocytoma | Moderately aggressive | Moderate (2 to 5 years) |
| Grade IV | Glioblastoma (GBM) | Highly aggressive, infiltrative | Poor (12 to 18 months median) |
As this table makes clear, pilocytic astrocytoma occupies the most favorable position in the entire spectrum. Its well-defined borders, benign growth pattern, and resistance to malignant change set it apart from every other glioma subtype. This distinction carries enormous implications for both treatment and prognosis.
Treatment Options for Pilocytic Astrocytoma
One of the reassuring aspects of pilocytic astrocytoma is that treatment does not always require the aggressive, multi-pronged approach used for high-grade gliomas. Instead, the management plan is carefully tailored based on the tumor’s location, the patient’s age, the presence or absence of symptoms, and the feasibility of surgery.
The Treatment Pathway
- Observation (Watch and Wait): For small, asymptomatic tumors, particularly optic pathway gliomas in NF1 patients, your medical team may recommend close monitoring with periodic MRI scans rather than immediate intervention. This approach avoids the risks of surgery when the tumor is not causing problems and may never do so.
- Surgical Resection: By far the most important and most effective treatment. When the neurosurgeon achieves gross total resection (meaning the entire visible tumor is removed), the chance of long-term cure exceeds 95 percent. As a result, surgery remains the cornerstone of treatment planning. Advanced neurosurgical techniques available today make this goal achievable in a growing number of cases.
- Chemotherapy: Reserved for situations where surgery cannot safely remove the entire tumor or when the disease comes back after initial treatment. The carboplatin-vincristine combination has been the standard first-line regimen for decades, and newer targeted drugs (discussed below) are now expanding the therapeutic toolbox.
- Radiation Therapy: Because of the risks that radiation poses to the developing brain, it is generally treated as a last resort, particularly in children. That said, focused radiation techniques may be appropriate for older adolescents or adults with recurrent, treatment-resistant tumors.
- Targeted Molecular Therapy: With the discovery of BRAF alterations in the vast majority of pilocytic astrocytomas, drugs that specifically block these molecular pathways are showing real promise. This approach represents a shift toward precision medicine: treating the tumor based on its genetic makeup rather than its location alone.
Microsurgical Resection: The Gold Standard
There is broad consensus in the neurosurgical community that surgery is the single most important factor in determining outcomes for pilocytic astrocytoma patients. When a skilled neurosurgeon achieves gross total resection, the tumor is effectively cured in the vast majority of cases. This is a statement that applies to very few other brain tumors.
Naturally, the challenge lies in removing as much tumor as possible while protecting the brain’s critical functions. This is where modern surgical technology makes a real difference. At our center, advanced glioma neurosurgery relies on several key tools:
- Intraoperative Neurophysiological Monitoring (IONM): Electrodes placed on the patient’s body continuously track motor, sensory, and cranial nerve pathways throughout the operation. This real-time feedback acts as an early warning system, alerting the surgeon the moment a critical pathway is at risk.
- Frameless Neuronavigation: Before surgery, the patient’s MRI data is loaded into a navigation system that functions much like a GPS for the brain. During the operation, the surgeon can see exactly where the instruments are in relation to the tumor and surrounding structures, enabling millimeter-level precision.
- Operative Microscopy: High-powered microscopes with adjustable magnification and lighting allow the surgeon to clearly distinguish tumor tissue from normal brain, which is especially important near the tumor margins where the boundary may be subtle.
- Intraoperative MRI: In selected cases, a mid-surgery MRI scan can reveal whether any residual tumor remains before the operation is completed, giving the surgeon a second chance to achieve complete removal.
- Ultrasonic Aspiration (CUSA): This specialized instrument uses ultrasonic vibrations to gently break apart and suction tumor tissue while leaving adjacent normal brain largely undisturbed. It is particularly valuable when operating near eloquent brain areas.
What the Numbers Show: Surgical Outcomes by Location
| Tumor Location | Complete Removal Rate | Recurrence Risk | 10-Year Disease Control |
|---|---|---|---|
| Cerebellum | 85 to 95% | Low (5 to 10%) | Over 90% |
| Optic Pathway | 10 to 30% | Moderate (30 to 40%) | 70 to 80% |
| Brainstem | 40 to 70% | Low to Moderate (15 to 25%) | 80 to 90% |
| Cerebral Hemispheres | 70 to 90% | Low (5 to 15%) | Over 85% |
| Spinal Cord | 50 to 70% | Low to Moderate (10 to 20%) | 80 to 90% |
Chemotherapy, Radiation, and Emerging Targeted Therapies
Although surgery alone is often sufficient, there are clinical scenarios where additional treatment becomes necessary. The decision to add chemotherapy or radiation depends on several factors, including the extent of surgical removal, the tumor’s location, the patient’s age, and whether the disease shows signs of progression over time.
Chemotherapy
The carboplatin and vincristine (CV) regimen has served as the backbone of medical therapy for pilocytic astrocytoma for over two decades. Studies have demonstrated response rates in the range of 50 to 60 percent, and the treatment is generally well tolerated in pediatric patients, though clinicians must watch for side effects such as low blood counts, peripheral nerve irritation, and occasional allergic reactions to carboplatin.
More recently, however, a wave of targeted drugs has begun to change the landscape:
- MEK Inhibitors (Selumetinib, Trametinib): These drugs block a signaling cascade called the MAPK/ERK pathway, which is overactivated in pilocytic astrocytomas because of their BRAF alterations. Clinical trials have produced encouraging results, and regulatory approvals for specific indications are progressing.
- BRAF Inhibitors (Dabrafenib): Particularly effective against the subset of tumors carrying the BRAF V600E mutation. These can be used alone or combined with MEK inhibitors for a dual-blockade strategy.
- Vinblastine Single-Agent Therapy: An alternative maintenance option with a relatively mild side-effect profile, sometimes preferred for long-term management.
Radiation Therapy
Given the significant long-term risks associated with brain irradiation, including cognitive decline, hormonal disruption, growth impairment, blood vessel damage, and a small but real risk of secondary cancers, radiation is generally avoided in children with pilocytic astrocytoma. Exceptions include:
- Tumors that continue to grow despite multiple rounds of chemotherapy
- Adult patients where surgical options are limited
- Focused techniques such as stereotactic radiosurgery for small, well-defined residual tumor
When radiation becomes necessary, newer modalities such as proton beam therapy offer a meaningful advantage. Because protons deposit most of their energy at a precise depth and then stop, the surrounding healthy brain receives far less incidental radiation compared with conventional photon-based treatment.
Prognosis and Survival Data
Among all brain tumors, pilocytic astrocytoma carries the most favorable prognosis. This is not merely a comforting talking point; the data consistently supports it across multiple large-scale studies spanning decades of follow-up.
Survival at a Glance
- 5-Year Overall Survival: Greater than 96 percent
- 10-Year Overall Survival: Greater than 94 percent
- 20-Year Overall Survival: Greater than 90 percent
- Cure Rate After Complete Removal: Approximately 95 percent
- Recurrence After Complete Removal: Only 5 to 10 percent
- Risk of Malignant Transformation: Under 2 percent
What Influences the Outcome?
- Completeness of Surgery: This is, without question, the most powerful predictor. Patients who undergo gross total resection enjoy cure rates above 95 percent, while those with residual tumor face a higher, though still manageable, risk of recurrence.
- Tumor Location: Cerebellar tumors yield the best results because they are most amenable to complete removal. Conversely, optic pathway and hypothalamic tumors present greater surgical challenges and generally have somewhat lower rates of disease-free survival.
- Age at Diagnosis: Very young children, particularly infants, may carry a modestly higher recurrence risk. Adult pilocytic astrocytomas, while uncommon, usually maintain similarly favorable outcomes.
- Molecular Profile: Tumors driven by the KIAA1549-BRAF fusion tend to follow a particularly indolent course. The BRAF V600E mutation, while also associated with generally good outcomes, may carry a slightly different biological trajectory.
- NF1 Status: Interestingly, NF1-associated optic pathway gliomas sometimes follow a remarkably indolent course, with some tumors stabilizing or even shrinking without any treatment at all.
Pilocytic Astrocytoma vs. Glioblastoma: Two Ends of the Spectrum
Patients and families frequently ask how pilocytic astrocytoma compares to glioblastoma multiforme, the brain tumor that receives the most public attention. While both arise from glial cells, the similarities essentially end there. The table below lays out the critical differences.
| Feature | Pilocytic Astrocytoma (Grade I) | Glioblastoma (Grade IV) |
|---|---|---|
| Growth Rate | Slow | Rapid and aggressive |
| Tumor Borders | Clear, well-defined | Diffuse, infiltrating normal brain |
| Typical Age Group | Children and young adults | Older adults (55 to 75 years) |
| Chance of Cure | High with complete surgery | Very low |
| 10-Year Survival | Over 94 percent | Under 5 percent |
| Standard Treatment | Surgery, often curative alone | Multimodal (surgery + radiation + chemotherapy) |
| Role of Immunotherapy | Not typically needed | NK cell therapy under active investigation |
This comparison underscores a vital point: accurate diagnosis and proper tumor grading are absolutely essential. The treatment path and expected outcome for a Grade I pilocytic astrocytoma is worlds apart from that of a Grade IV glioblastoma, and each requires its own tailored approach.
Long-Term Outlook and Follow-Up After Treatment
For the great majority of pilocytic astrocytoma patients, the years following treatment bring welcome normalcy. Children return to school, re-engage with friends and sports, and go on to lead full, productive lives. However, ongoing surveillance remains an important part of the long-term care plan, primarily to catch any recurrence early, even though recurrence is uncommon.
Recommended Monitoring Schedule
- Years 1 through 2: MRI scans every 3 to 6 months
- Years 3 through 5: Annual MRI scans
- Beyond 5 years: Annual or biennial imaging based on clinical judgment and resection extent
- NF1 patients: More frequent follow-up, including annual ophthalmologic exams
Quality of Life Considerations
While most patients recover fully, certain aspects of long-term health deserve ongoing attention:
- Cognitive Monitoring: Baseline and periodic neuropsychological testing helps detect any subtle changes in memory, attention, or processing speed before they become noticeable in daily life.
- Hormonal Health: Patients who had tumors near the hypothalamus or who received radiation should have regular endocrine evaluations to catch hormonal deficiencies early.
- Vision Care: Those treated for optic pathway tumors benefit from structured visual rehabilitation and regular ophthalmologic assessments.
- Emotional Wellbeing: A brain tumor diagnosis leaves emotional footprints on patients and families alike. Access to counseling, peer support, and patient communities can make a real difference during recovery and beyond.
- Physical Rehabilitation: Targeted physiotherapy and occupational therapy help patients regain coordination, strength, and confidence in their physical abilities after surgery.
Expert Insight: Prof. Dr. Serdar Baki Albayrak
Decades of Experience in Brain Tumor Surgery
Prof. Dr. Serdar Baki Albayrak is a seasoned neurosurgeon whose career spans more than 27 years at the forefront of brain tumor management. His clinical practice encompasses the full spectrum of central nervous system tumors, from the most treatable Grade I pilocytic astrocytomas to the most complex glioblastoma multiforme cases.
Prof. Albayrak is a firm believer in the principle of maximum safe resection, and his surgical practice reflects this commitment. By integrating intraoperative neurophysiological monitoring, advanced imaging, and meticulous microsurgical technique, he consistently works to give each patient the best possible chance at a complete, function-preserving tumor removal.
His contributions extend beyond the operating room as well. Prof. Albayrak has been instrumental in advancing NK cell immunotherapy as a treatment option for patients with malignant gliomas. This pioneering approach trains the body’s own immune cells to recognize and attack tumor tissue. His integrated, multimodal care philosophy ensures that every patient receives a treatment plan crafted to their individual needs.
“Each brain tumor, regardless of its grade, demands the highest level of surgical precision and personalized care. Our mission is not just to treat the tumor; it is to help our patients reclaim their lives.”
Prof. Dr. Serdar Baki Albayrak
Schedule a Consultation
Our neuro-oncology team provides expert evaluation and individualized treatment planning for patients with all types of brain tumors.
Contact Us TodayFrequently Asked Questions About Pilocytic Astrocytoma
Q: What exactly is Grade I Pilocytic Astrocytoma?
It is a slow-growing, benign brain tumor that the World Health Organization classifies at the lowest grade on its four-tier scale. This tumor primarily develops in children and young adults, most often in the cerebellum, optic pathway, or brainstem. Among all brain tumors, it carries one of the most favorable prognoses, with long-term cure rates surpassing 95 percent when surgeons achieve complete removal.
Q: Can pilocytic astrocytoma be cured?
Yes, and this is one of the most encouraging aspects of this diagnosis. When the neurosurgeon is able to remove the tumor completely, the likelihood of permanent cure exceeds 95 percent. Even in cases where the tumor’s location prevents total removal, the overall outlook remains positive with careful monitoring and, when needed, targeted medical treatment.
Q: What symptoms should raise concern?
The symptoms depend largely on where the tumor is located, but the most common ones include persistent headaches (particularly in the morning), nausea or vomiting, balance difficulties, vision changes, and seizures. In young children, parents may also notice an increase in head size or a regression of developmental milestones. Because these symptoms tend to develop gradually, any persistent or worsening neurological complaint deserves medical evaluation.
Q: What is the primary treatment?
Surgical resection is the primary and most effective treatment. The goal is to remove the entire tumor while preserving neurological function. Modern microsurgical techniques with real-time nerve monitoring make safe, complete removal possible in the majority of cases. When complete resection is not feasible, chemotherapy or other medical therapies may be added.
Q: How does pilocytic astrocytoma differ from glioblastoma?
These two tumors sit at opposite ends of the brain tumor spectrum. Pilocytic astrocytoma is slow-growing, has clear borders, primarily affects children, and boasts survival rates above 94 percent at 10 years. Glioblastoma, on the other hand, is highly aggressive, infiltrates surrounding brain tissue, mainly strikes older adults, and carries a median survival measured in months rather than decades.
Q: Can the tumor come back after surgery?
Recurrence following complete surgical removal is uncommon, happening in roughly 5 to 10 percent of patients. The risk is higher when only partial removal was achieved. This is precisely why regular follow-up MRI scans are so important – they allow the medical team to detect any regrowth at the earliest possible stage. Even if recurrence does occur, the tumor typically stays low-grade and can usually be managed with a second operation.
Q: Is there a risk that it will turn into cancer?
Malignant transformation, meaning a change from Grade I to a higher, more aggressive grade, is extremely uncommon with pilocytic astrocytoma. Published data suggest this happens in fewer than 2 percent of cases. This is a key distinction from diffuse astrocytomas, which carry a meaningful risk of progressing to higher grades over time.
Q: How long is the recovery after surgery?
Most patients are well enough to leave the hospital within 5 to 7 days after the procedure. The full recovery timeline, including a return to school for children or work for adults, typically falls in the range of 4 to 8 weeks. This varies somewhat depending on the tumor’s location, the extent of the operation, and the patient’s baseline health. Physical therapy often plays a helpful role in speeding up recovery.
Q: Can adults get pilocytic astrocytoma?
They can, though it is considerably less common than in children. Adult pilocytic astrocytomas tend to appear in different locations, more often in the cerebral hemispheres or spinal cord rather than the cerebellum. Fortunately, the prognosis for adult patients is generally comparable to pediatric outcomes, especially when complete surgical resection is achieved.
Q: Does immunotherapy have a role in treating this tumor?
At present, immunotherapy approaches such as NK cell therapy are primarily being developed and applied for high-grade tumors like glioblastoma. Because pilocytic astrocytoma responds so well to surgery and frequently to surgery alone immunotherapy is not part of the standard treatment protocol for this tumor type. That said, researchers continue to explore immunological strategies for the rare cases that resist conventional treatment.
Conclusion: A Diagnosis That Carries Real Hope
In the world of brain tumors, Grade I Pilocytic Astrocytoma is genuinely good news. That may sound like an unusual thing to say about any brain tumor, but the evidence speaks for itself: with cure rates above 95 percent following complete surgical removal, this tumor offers patients and families a realistic path toward full recovery and a normal life.
Here is what matters most from everything covered in this guide:
- Pilocytic astrocytoma is the most common and most curable brain tumor in children
- Surgery is the primary treatment and is frequently curative on its own
- Modern microsurgical techniques with intraoperative monitoring enable safe, thorough tumor removal
- The risk of malignant transformation is extremely low, under 2 percent
- Long-term survival exceeds 94 percent at the 10-year mark
- Targeted molecular therapies are expanding the options for tumors that cannot be completely removed
- Regular MRI follow-up ensures any recurrence is caught early
If you or someone you care about has received this diagnosis, take some comfort in knowing that the medical community has extensive experience managing pilocytic astrocytoma, and that the outcomes, by brain tumor standards, are outstanding. The expertise of dedicated neurosurgeons like Prof. Dr. Serdar Baki Albayrak, combined with a thoughtful, comprehensive treatment plan, gives patients every reason for optimism.
Take the First Step Toward Expert Care
Our specialized neuro-oncology team is ready to provide thorough evaluation and personalized treatment planning for all brain tumor types.
Book a ConsultationLast reviewed: March 2026 | Reviewed by: Prof. Dr. Serdar Baki Albayrak, Neurosurgeon
Disclaimer: This article is intended for informational purposes and does not replace professional medical advice. Treatment decisions should always be discussed with your neurosurgical team based on your individual circumstances.